InService Insights: Fingertip amputations
Fingertip amputations are common injuries that, perhaps unsurprisingly, are well represented on the In-Service Exam each year. In order to help residents better-prepare for this section of the exam, this article will focus on the indications of each reconstructive modality, highlighting some the basic indications and limitations of the various reconstructive modalities for fingertip amputations. Those who would like to pursue a more in-depth discussion of technical details of these are encouraged to visit the "Suggested Reading" section at the end of this article.
Anatomy
The fingertip is defined by the distal phalanx and soft tissue distal to the insertion of the flexor and extensor tendons. The nail bed is tightly adherent to the distal phalanx and is composed of the germinal and sterile matrices. It's bordered by the eponychium proximally, paronychium laterally and hyponychium distally. Vascular supply is from the proper digital vessels, which arborize past the level of the DIP joint.
Evaluation
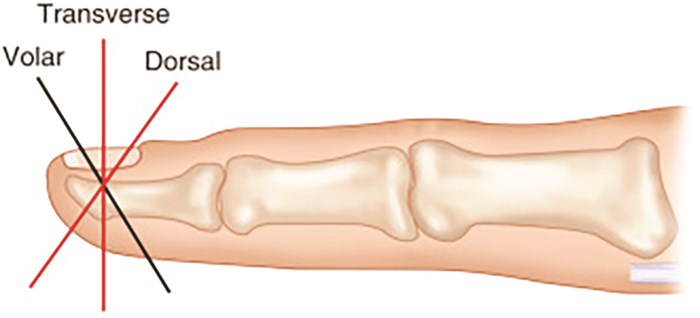
Fingertip injuries are best approached in an algorithmic fashion dictated by the injury geometry (Fig. 1), defect size and presence of exposed bone or tendon. The functional priorities of each digit should also be taken into account. For example, reconstructive options that allow for preservation of sensation are preferred for the thumb and index, which serve a primary precision function. Maintenance of length is the priority for the middle finger; thus, sacrificing considerable length for sensation may not be the optimal choice. As the ulnar digits play a primary role in power grip, reconstructions that preserve joint mobility and provide a flexor surface devoid of potentially painful scars are favored.
Salvage vs. Revision Amputation
Generally, injuries proximal to the lunula are best treated with a revision amputation. Additionally, some patients may prefer an amputation, the classic example of which is a laborer who favors an expedited return to work at the expense of a shortened digit. In pediatric patients, the amputated part can be replaced as a composite graft, though the published success rates are highly variable.
Secondary Intention, Skin Grafts
Injuries ≤1.5cm2 without exposed bone or tendon can be left to heal secondarily with excellent sensation and functional outcomes. Exposed distal phalanx can be conservatively shortened to allow for secondary intention, but shortening should not exceed the distal-most aspect of the nail bed to prevent a hook-nail deformity. For defects >1.5cm2, split- and full-thickness skin grafts can be used, and patients may recover protective sensation, but can result in cold intolerance.
Flap Options (Index, Middle, Ring, Small)
Exposed bone or denuded tendon are indications for flap coverage if salvage is desired. The flap options can be broadly categorized as local, homodigital or heterodigital flaps. Local flaps allow for excellent preservation of sensation but are typically limited to smaller defects (≤1cm). Homodigital flaps also provide good sensory outcomes and can be applied to larger defects (≤2cm), but often require shortening of the digit to achieve adequate coverage. For even larger defects, heterodigital flaps can be used, but these have the poorest sensory outcomes amongst the flap options.
Local Flaps
The volar V-Y flap (Atasoy) can be used for dorsal-oblique and distal-transverse amputations on any digit. The apex of the flap typically extends to the distal flexion crease resulting in advancement up to 1cm. Bilateral V-Y advancement flaps, described by Kutler, can be used for transverse and lateral-oblique amputations, but result in a scar at the volar fingertip. For lateral-oblique injuries with exposed bone, a lateral pulp flap can provide bony coverage by mobilizing the adjacent volar pulp to allow for healing by secondary intention.
Homodigital Flaps
The oblique triangular neurovascular island flap is an axial flap, based on one of the proper digital neurovascular bundles, and can provide coverage of volar-oblique, lateral-oblique, and transverse defects up to 2cm. Extending the apex of the flap proximal to the PIP joint affords greater mobility for advancement. The Hueston flap is a laterally based, volar rotation-advancement flap with a proximal back cut that can be used for transverse amputations. Reverse-flow homodigital island flaps take advantage of the anastomoses between the radial and ulnar digital arteries at the interphalangeal joint spaces, allowing for a distally based flap nourished by the contralateral digital artery. The digital nerve can be left in situ or, for a sensate flap, incorporated in the flap and coapted to the contralateral digital nerve.
Heterodigital Flaps
The thenar flap is an option for larger defects of the index finger - but it's particularly attractive for the middle finger, as it reliably allows for preservation of length. It's contraindicated in patients with a high risk for developing joint contractures. The cross-finger flap can be used for volar defects of the ring and small fingers, where the primary goal is preservation of power grip, so preservation of IP joint mobility and absence of volar scars are ideal. Contrarily, for dorsal defects of the digits, a reverse cross-finger flap may be utilized.
Thumb
The Moberg flap is an axial advancement flap that provides excellent sensation and can resurface volar defects up to 1-1.5cm (Fig. 4). Because both neurovascular bundles are included in the flap, its use is reserved for the thumb due to a reliable dorsal blood supply via the princeps pollicis that prevents dorsal skin necrosis. Flap advancement may require slight IP joint flexion, which can result in contracture, although this is rare. The flap can be islandized to provide another 0.5cm of advancement, or extended onto the thenar eminence (Dellon modification) to allow reconstruction of defects up to 3cm. For thumb defects >3cm, the first dorsal metacarpal artery (FDMA) flap can be used. It's taken from the dorsum of the index finger overlying the proximal phalanx. Inclusion of a superficial sensory branch of the radial nerve provides a sensate flap, though cortical retraining is necessary. The Littler neurovascular island flap, based off the ulnar surface of the middle finger, can also be used for defects >3cm; however, significant donor site morbidity limits the use of this flap in common practice.
Suggested Reading
Lemmon JA, Janis JE, Rohrich RJ. Soft-tissue injuries of the fingertip: methods of evaluation and treatment. An algorithmic approach. Plast Reconstr Surg. 2008 Sep;122(3):105e-117e.
Lee DH, Mignemi ME, Crosby SN. Fingertip injuries: an update on management. J Am Acad Orthop Surg. 2013 Dec;21(12):756-66.
Martin C, Gonzalez del Pino J. Controversies in the treatment of fingertip amputations. Conservative versus surgical reconstruction. Clin Orthop Relat Res. 1998 Aug;(353):63-73.
Mailey B, Neumeister MW. The fingertip, nail plate and nail bed: Anatomy, repair, and reconstruction. In: Chang J, Neligan P, eds. Plastic Surgery: Volume 6: Hand and Upper Extremity. Elsevier, Inc.; 2017:122-145.